Rectal prolapse is a condition that can be both physically uncomfortable and emotionally distressing. Although it may feel difficult to discuss, early diagnosis and treatment can greatly improve a patient’s quality of life. At Park Avenue Colon and Rectal Surgery, we specialize in diagnosing and treating rectal prolapse with expertise, precision, and compassion.
Below, we break down what rectal prolapse is, why it occurs, how it’s treated, and what you can expect from professional care.
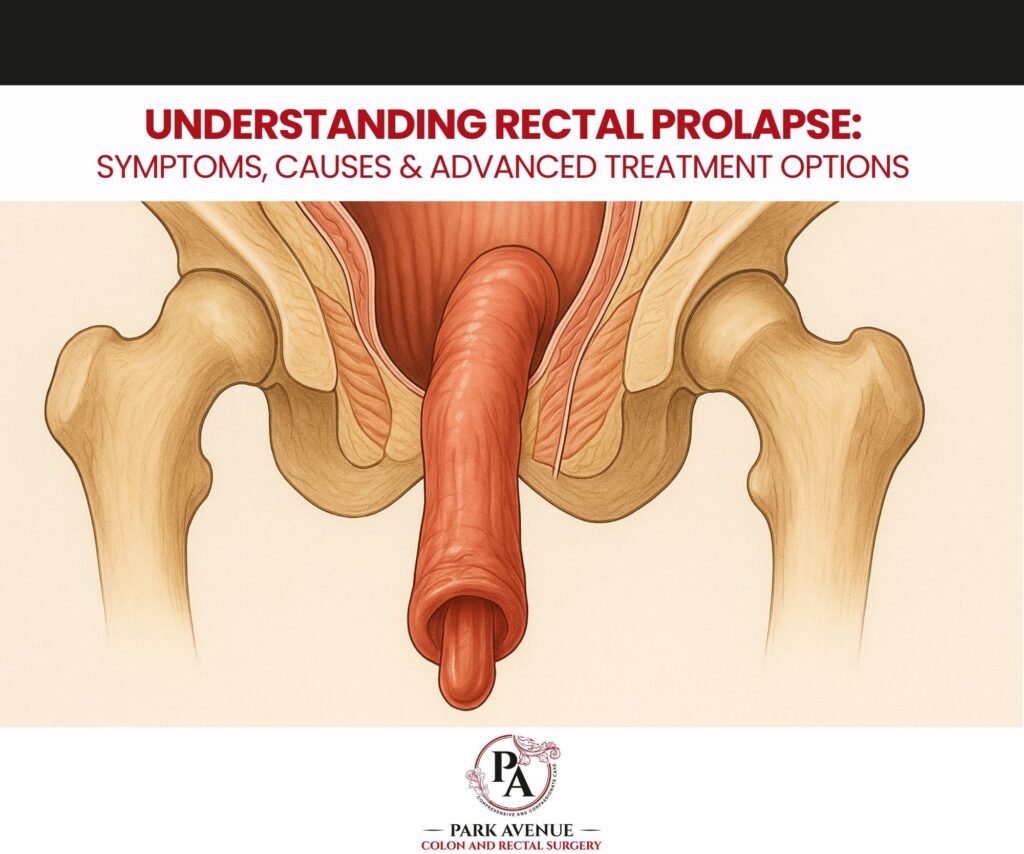
What Is Rectal Prolapse?
Rectal prolapse occurs when the rectum—the last part of the large intestine—slips or protrudes through the anal opening. It may start subtly but can progress over time.
There are three types:
- Internal Prolapse: The rectum folds into itself without exiting the anus.
- Partial (Mucosal) Prolapse: Only the inner lining of the rectum protrudes.
- Full-Thickness Prolapse: The entire rectal wall protrudes outside the body.
Though more common in older adults, rectal prolapse can affect people of any age.
Common Symptoms
Many early symptoms resemble hemorrhoids, making evaluation essential. Patients may experience:
- A bulge or protrusion from the anus
- Difficulty with bowel movements or incomplete evacuation
- Mucus leakage
- Fecal incontinence
- Bleeding
- Chronic constipation
- A persistent sensation of rectal fullness
If you notice these signs, a medical evaluation is recommended.
What Causes Rectal Prolapse?
Rectal prolapse is usually linked to weakened pelvic floor muscles and connective tissues. Contributing factors include:
- Chronic constipation or straining
- Pregnancy and childbirth
- Aging
- Long-term diarrhea
- Neurological disorders
- Prior pelvic or anorectal surgery
- Pelvic floor dysfunction
Understanding the underlying cause is key to developing an effective treatment plan.
Diagnosis at Park Avenue Colon and Rectal Surgery
Evaluation typically includes:
- A thorough medical history and physical exam
- Anorectal manometry to assess muscle function
- Defecography to study pelvic floor movement
- Colonoscopy to rule out other conditions
- Imaging studies (MRI or CT) for complex cases
This comprehensive approach ensures accurate diagnosis and personalized treatment.
Treatment Options
Treatment varies depending on severity and patient factors.
Non-Surgical Management (Early Stages)
While these methods may reduce symptoms, they typically do not cure prolapse:
- Increasing dietary fiber
- Staying well hydrated
- Pelvic floor therapy
- Using stool softeners
Surgical Treatment (Definitive Solution)
Surgery is considered the most effective treatment for full-thickness or symptomatic prolapse.
Abdominal Rectopexy (Often Minimally Invasive)
The rectum is repositioned and secured using laparoscopic or robotic techniques. Benefits include:
- Small incisions
- Faster recovery
- Lower recurrence rates
Perineal Procedures
Performed through the anus—typically recommended for older or medically complex patients:
- Altemeier procedure
- Delorme procedure
Dr. Marsha Harris will determine the best surgical approach based on anatomy, health status, and patient goals.
Recovery & Prognosis
Most patients experience:
- Significant symptom relief
- Improved bowel function
- Increased comfort and mobility
- Reduced incontinence
With modern surgical techniques, recurrence is low and long-term outcomes are positive.
Rectal Prolapse: Frequently Asked Questions
Q: Is rectal prolapse the same as hemorrhoids?
A: No. Hemorrhoids involve swollen blood vessels; rectal prolapse involves part of the rectum slipping out of place.
Q: Can rectal prolapse resolve without treatment?
A: Mild cases may temporarily improve, but full-thickness prolapse will not resolve without medical or surgical intervention.
Q: What increases the risk?
A: Aging, chronic constipation, multiple childbirths, pelvic floor dysfunction, and neurological conditions all increase risk.
Q: Will I need surgery?
A: Surgery is the only definitive treatment for full-thickness prolapse, but mild cases may be managed symptomatically.
Q: How long is the recovery after surgery?
A: Many patients resume normal activities within 1–3 weeks, depending on the procedure.
Q: Can I regain bowel control?
A: Yes. Many patients experience improved continence after corrective surgery.
Q: When should I see a specialist?
A: Seek consultation if you notice protrusion, difficulty with evacuation, leakage, or persistent discomfort.
Contact Information
Park Avenue Colon and Rectal Surgery
📍 36 E 36th St, Suite 1C
New York City, NY 10016
📞 Phone: (646) 822-0228
🌐 Website: marshaharrismd.com
🗓 Appointments: https://marshaharrismd.com/appointments